
The healthcare system in Taiwan has been highly specialized. However, with an early step into a super-aged society, this kind of highly-specialized healthcare system begins to reveal an inadequacy in the traditional mode of human resources distribution in the face of worsening burden arising from patients with chronic disease.
To balance the distribution of medical resources and lessen the burden of the healthcare system, levels of care are being planned with an emphasis on the vertical integration services among different levels of hospitals and communal medical groups. Ward service in hospitals is also undergoing a reformation.
In Taiwan, hospitalist medicine is the solution for a super-aged society. The hospitalist system was first introduced to Chang Gung Memorial Hospital (CGMH) in 2002, establishing the foundation for hospitalist medicine. In October 2009, specialized acute care wards were set up by Dr. Ko Wen-Je at National Taiwan University Hospital (NTUH) to raise the overall quality of medical care.So far, 19 hospitals in Taiwan have established specialized hospitalist wards. In February 2019, Taiwan Association of Hospital Medicine was founded with the membership of 180 specialized doctors with hospitalist-care certification, who are consistently undergoing training and attending international conferences.

So far, 19 hospitals in Taiwan have established specialized hospitalist wards. In February 2019, Taiwan Association of Hospital Medicine was founded with the membership of 180 specialized doctors with hospitalist-care certification, who are consistently undergoing training and attending international conferences.
Four Paradigm Shifts by Hospitalists in Taiwan
A.Accountability
Hospitalists are medical specialists focusing on the care of hospitalized patients. In an aged society, patients with multiple diagnoses are ubiquitous, which would lead to difficulties under a highly-specialized healthcare system. However, for patients with a common diagnosis, hospitalists can integrate the medical instruments used by doctors with different specializations, such as POCUS (Point-of-Care Ultrasound) for a systematic evaluation, thus stepping toward providing holistic care.
B.Quality and patient safety
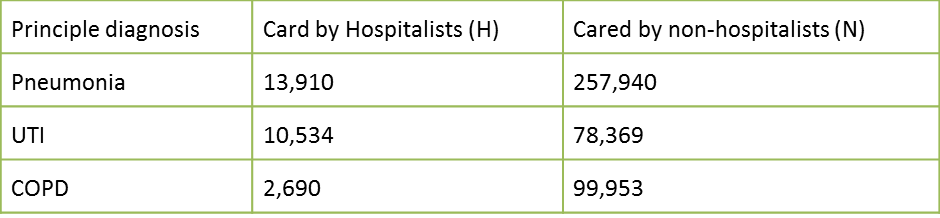
Doctors from which medical department are best for taking care of pneumonia patients or patients with urinary tract infection (UTI)? In Taiwan, hospitalists should be the answer. The following statistics from 2010 through 2014 shows the number of patients with common diseases, such as pneumonia, UTI, and COPD, as cared by hospitalists or cared by non-hospitalists in Taiwan.
The hospital mortality rates have declined under the care of hospitalists, which is more impressive given that patients receiving care by hospitalists were usually more sick. A prominent number of pneumonia patients suffer from other diseases or negative situations at the same time, for instance, critical illness (18.6% vs. 15.2%), stroke (11.5% vs.9.6%), diabetes (22.2% vs. 19.5%), low income status (4.8% vs. 2.6%).
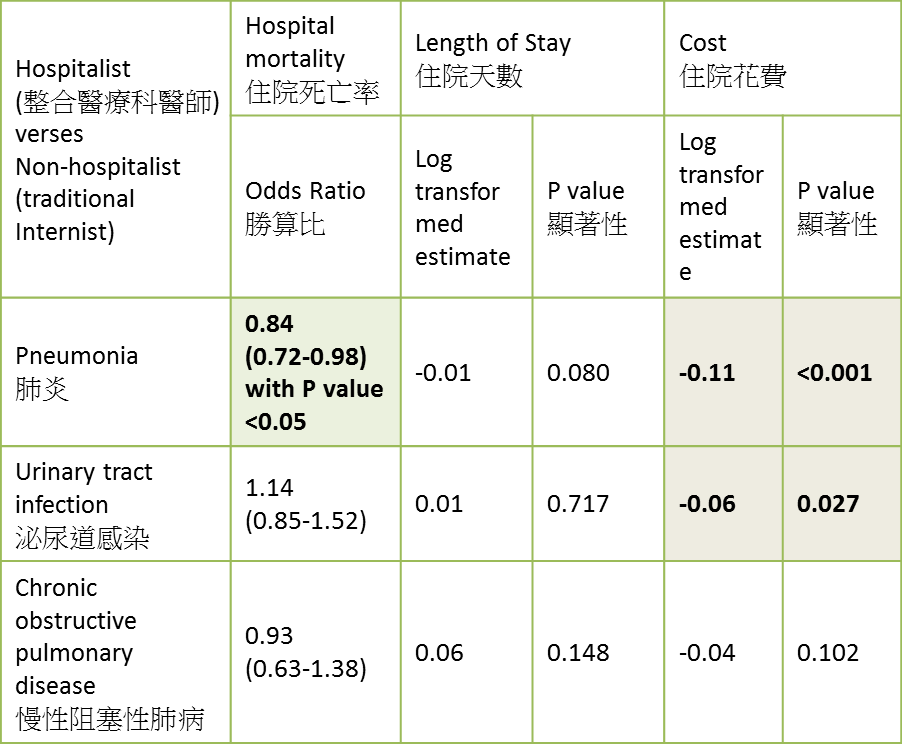
Post-discharge mortality rates of UTI patients have also decreased under the care of hospitalists. Furthermore, patients who suffer from pneumonia, UTI, and COPD under the care of hospitalists have performed better 30 days after discharge.

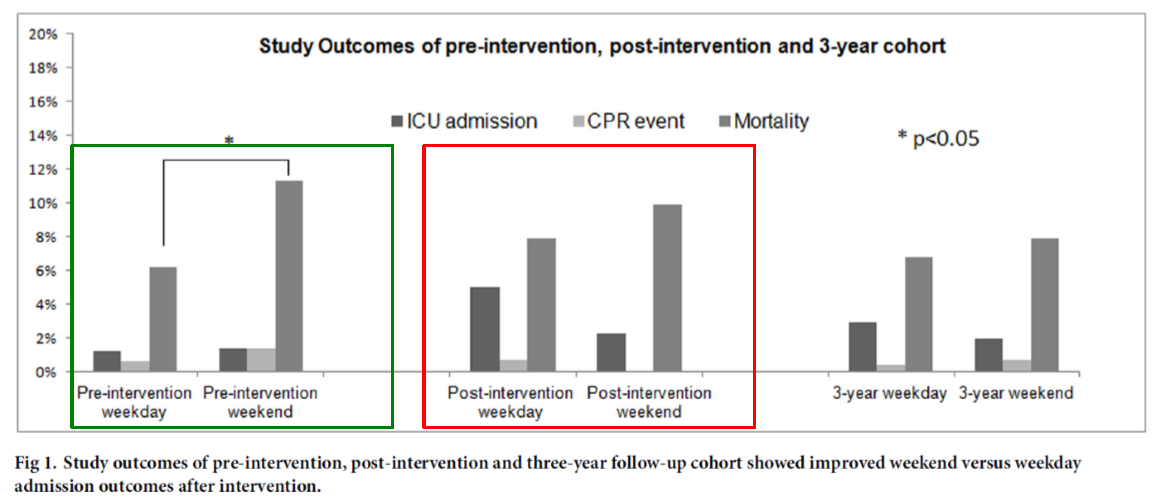
Medical specialists under hospitalist system works in shifts. Thus, proper staff number is maintained without causing weekend effect present in the traditional shift system.
C.Work-life balance
Presently, burnout and moral injury are the major threats to the health of medical specialists and thus the patients. Hospitalists hope to improve the shift system in the wards so that they can better focus on caring for the patients.
D.Choosing wisely
With a focus on providing holistic care and effective communication with the patients, the hospitalist system can reduce costs from every perspective. Aside from raising the quality of hospital care and patient satisfaction, the hospitalist system can also provide integrated outpatient care to patients with multiple chronic diseases. Special cases that require a surgery but rejected by the surgical department can be covered by the hospitalist system, serving as a crucial support of local medical network.
Hospitalists wards in community hospitals play a crucial role by emphasizing post-acute care (PAC). Many senior patients remain disabled after the treatment course of acute diseases, which is a common issue in an aged society. In 1984, Diagnosis Related Group (DRG) regulations were implemented in hospitals in the US, boosting the development of PAC institutions. On the other hand, the UK tackled the issue with the concept of intermediate care. Since 2014, National Health Insurance Administration in Taiwan has been working on PAC project for stroke patients. The project was expanded in 2017, providing care to patients suffering from stroke, burns, traumatic nerve injury, fractures resulted from osteoporosis, and heart failure.
In Taiwan, the PAC project has focused on expedient recovery and integrated care and rehabilitation with the coordinated effort of teams with various specializations including medicine, nursing, physical therapy, occupational therapy, language/dysphagia treatment, psychotherapy, social work, medical counseling, health education, complication prevention and control, working toward patients’ recovery in 2-3 weeks. The PAC project has eased the burden of families and the society, raised the efficiency of acute medicine, and bridged with long-term care.
Hospitalist System Effectively Reduces Readmission
Following global trend and the reduction of labor in hospitals, NTUH has initiated its own hospitalist system by the end of 2009. An integrated procedure that traced the recovery of the patients for a month after their discharge was implemented with details including preparations before discharge, condition tracing after discharge, telephone counseling service, hospitalist outpatient service, with a view to reducing the chances of readmission.
The NTUH hospitalist system was implemented from December 2009 to May 2010, 94 patients were traced in the first 60 days while 214 were traced in the later 120 days. There were 52 cases of unexpected readmission, three unexpected deaths, while another 50 could not be reached. Following the aforementioned procedure, both readmission and unexpected deaths within 30 days after discharge have decreased (25.5% vs. 14.6%, p = 0.021 by log-rank test). Tracing the patients through video chat or home visits should be the next steps to further enhance medical care in Taiwan.
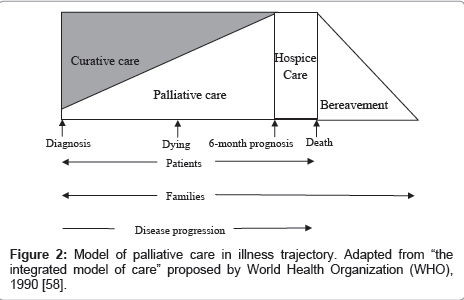
How Hospitalist Care Bridges with Hospice Care
Evaluation shall be conducted according to the Palliative Performance Index (PPI score) before providing hospice care to the patient with a focus on the psychological aspects of the patient. Psychological support and follow-up counseling for the patient’s family members are also emphasized.
Woman photo created by tirachardz






